






")
CP-Study
Effect of Vojta Therapy in children with cerebral palsy: a pilot study
Is Vojta Therapy (VT) an effective treatment for children with cerebral palsy (CP) using intermittent centre-based intensive blocks of treatment combined with daily treatment at home?
Fionn Bayley: Sozial Pädiatrisches Zentrum, DRK-Kinderklinik Siegen
Methods:
We used the Gross Motor Function Measure scores (GMFM-66) and normative GMFM-66 percentiles to detect the within-child improvement in gross motor capacity and relative ranking/change over time respectively.
Participants comprised 13 children with CP (spastic unilateral n=4, spastic bilateral n=7, dyskinetic n=2) in Gross Motor Function Classification Scale (GMFCS) Level I (n=3), Level II (n=2) and Level III (n=8), aged 2-11 years from various foreign countries who visited our centre 2-3 times a year for a 2-week intensive block of VT with an emphasis on parent instruction. Each child received two 45 minute VT treatments per day, 5 days/week. Parents carried out a 3rd treatment alone and over the weekend to consolidate their skills. At home each child was treated 2-4 times/day.
All the GMFM-66 assessments were carried out by the same 2 therapists trained in the administration and scoring of the GMFM. The change in percentiles between each child’s first 2 consecutive assessments (Tests 1 & 2) for GMFCS Level I, II and III were calculated. The median times between these 2 assessments were 1.1, 1.2, & 1.2 years for Levels I, II, and III respectively. The GMFM-66 percentiles by age for each GMFCS level were calculated from the table by Hanna*1. Data for the children in our study were analysed according to the GMFCS level allocated at the initial assessment*2.
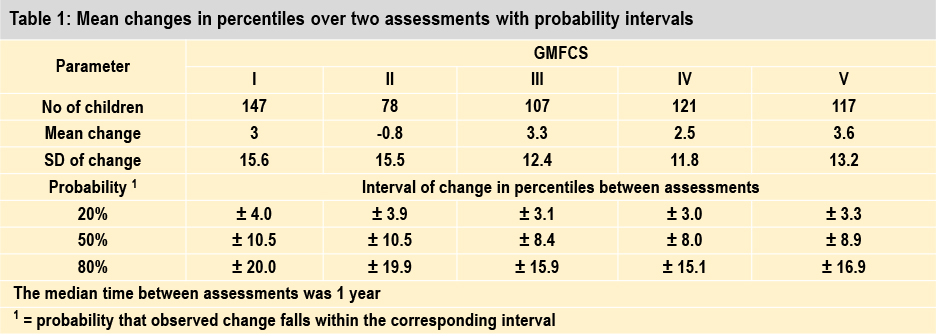
Expected within-child variability in percentiles:
The table from Hanna et al. (2008) shows intervals of expected change between 2 percentile measurements, corresponding to 20%, 50% and 80% coverage probabilities*3. The median time between measurements for each child was 1.0 year for each level*3.
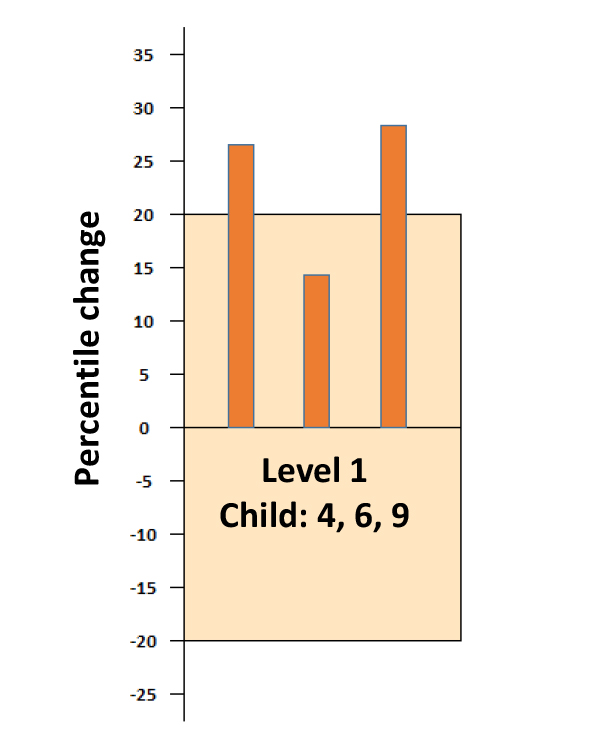
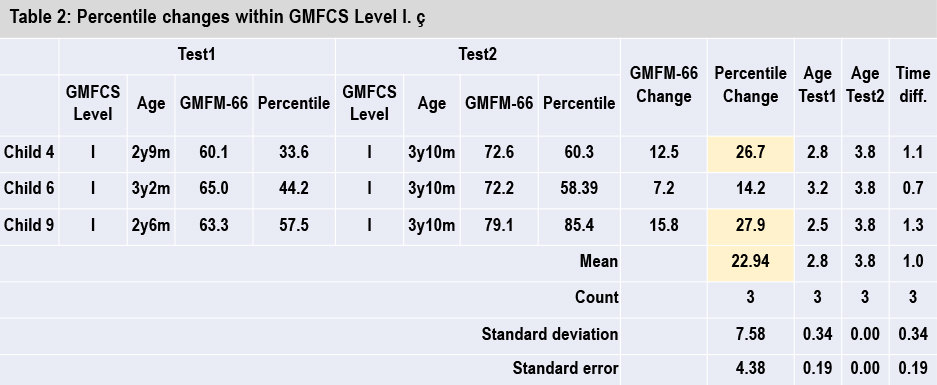
Results Level 1:
From Table 1. we see there is an 80% chance that the percentiles for children in level I will not change more than ± 20.0 points on retesting after 1 year. In Table 2, 2 from 3 children in Level I (child 4, 6 and 9) show much higher values (mean = 22.94, sd = 7.58) indicating their development was better than expected over the preceding year (median = 1.1y). No Z-statistic is calculated as the sample size is too small.
Copyright: Internationale Vojta Gesellschaft e.V.
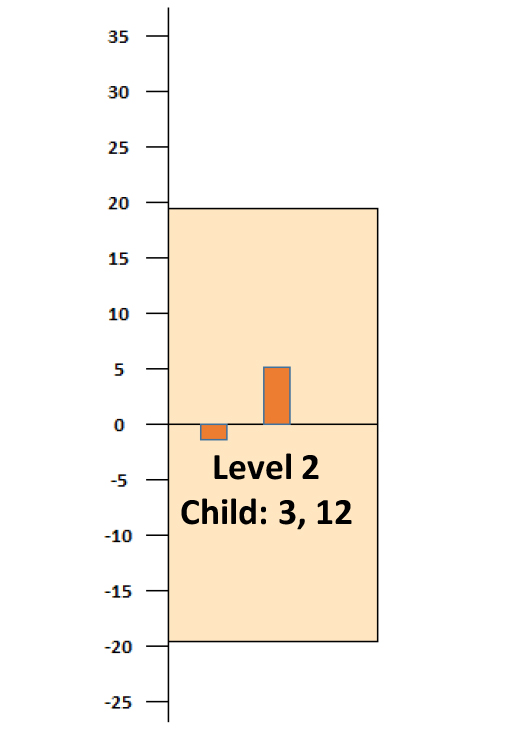
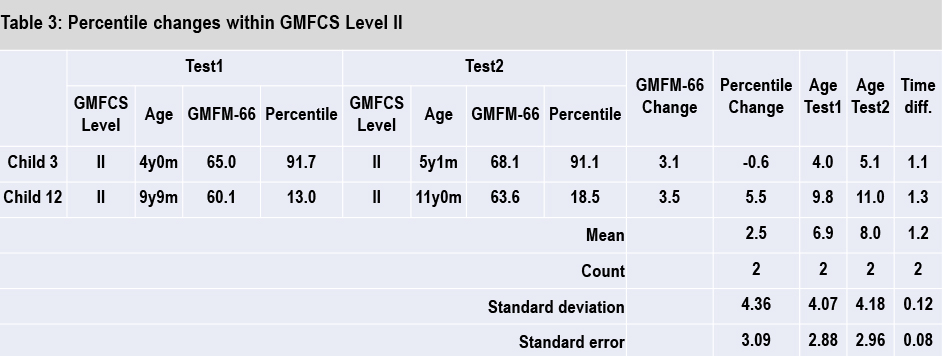
Results Level 2:
Both children in Table 3. show usual development in context to other children with CP in GMFCS level II. Our results could perhaps be explained by the findings from Palisano et al. – children classified at level II approached their maximum GMFM score more slowly than children classified at level I or at Level III*4.
Copyright: Internationale Vojta Gesellschaft e.V.
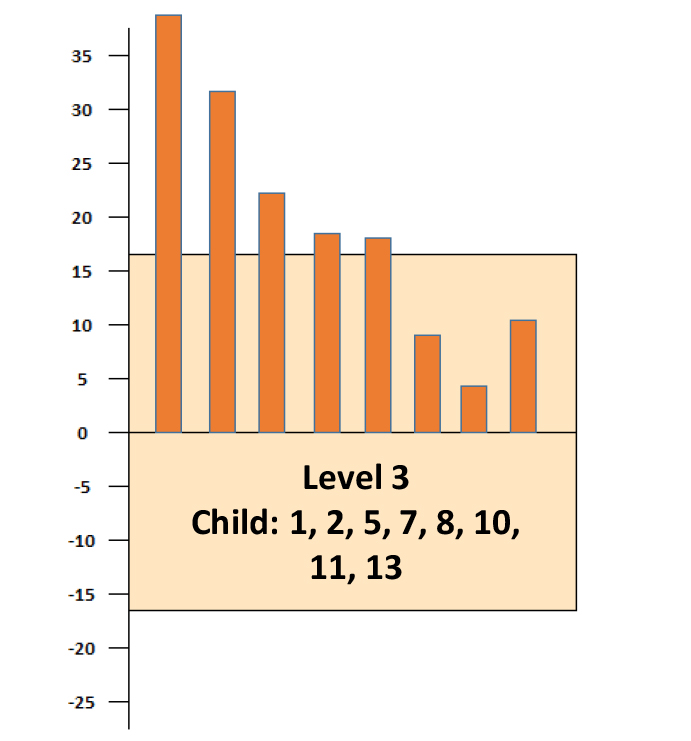
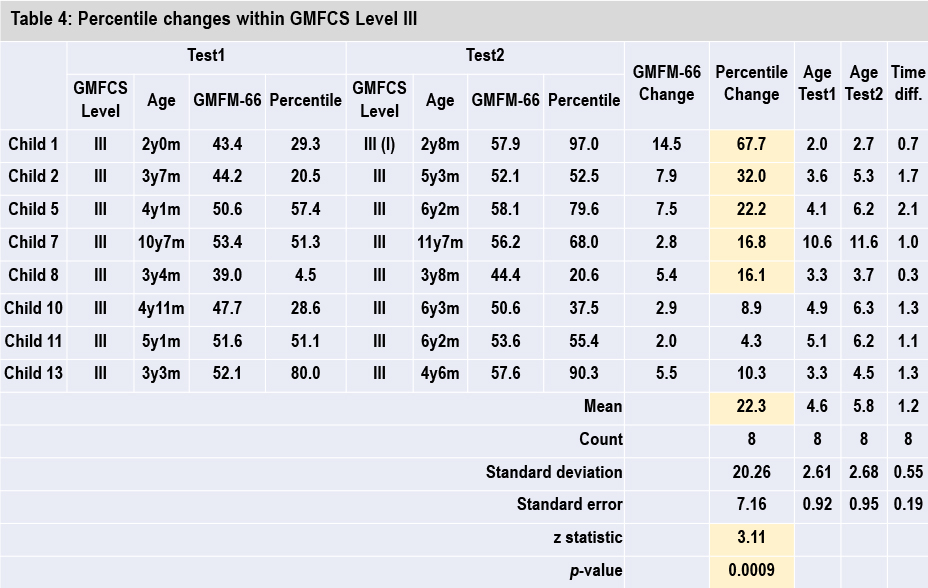
Results Level 3:
From Table 1. we see there is an 80% chance that the percentiles for children in level III will not change more than ± 15.9 points on retesting after 1 year*3. In Table 4, Child 1, 2, 5, 7 and 8 show higher values (mean = 22.3, sd = 20.26) indicating their development was better than expected over the preceding year (median = 1.2y). The change in percentile values for Level III is highly significant (p = 0.0009). Caution must be applied in interpreting these results due to the very small sample size.
Copyright: Internationale Vojta Gesellschaft e.V.
*1 GMFM-66 percentiles by age table from Steven Hanna (2008).
*2 Rosenbaum et al. 2002. Prognosis for Gross Motor Function in Cerebral Palsy: Creation of Motor Development Curves. JAMA 288: 1357-1363.
*3 Hanna et al. 2008. Reference Curves for the GMFM: Percentiles for Clinical Description and Tracking Over Time Among Children With Cerebral Palsy. Physical Therapy 88: 596-607
*4 Palisano et. al. 2000. Validation of a Model of Gross Motor Function for Children with Cerebral Palsy. Physical Therapy 80: 974-985.
Bolster et al. 2013. Long term effect of selective dorsal rhizotomy on gross motor function in ambulant children with spastic bilateral cerebral palsy, compared with reference centiles
Russell et al. 2000. Improved Scaling of the Gross Motor Function Measure for Children with Cerebral Palsy: Evidence of Reliability and Validity. Physical Therapy 80: 873-885.